GLP-1 Success Story
GLP-1 agonists (also called GLP-1RAs), and related drugs like dual agonists of gastric inhibitory polypeptide (GIP)/GLP-1, have revolutionized obesity treatment by demonstrating significant and sustained weight loss in clinical trials and real-world use. Drugs like semaglutide (Wegovy®) and tirzepatide (Zepbound®) have shown to improve efficacy compared to older weight-loss medications, with patients losing up to 20% of their body weight.
Their widespread adoption (a market size over $40 Billion USD in 2024) reflects their utility and demand, and there are early indications that they could be effective in other therapeutic areas. Riding the success in obesity, Eli Lilly announced that they would begin pursuing large studies to determine if GLP-1 agonists reduce alcohol abuse and drug use.
Current and Pipeline GLP-1 Agonists
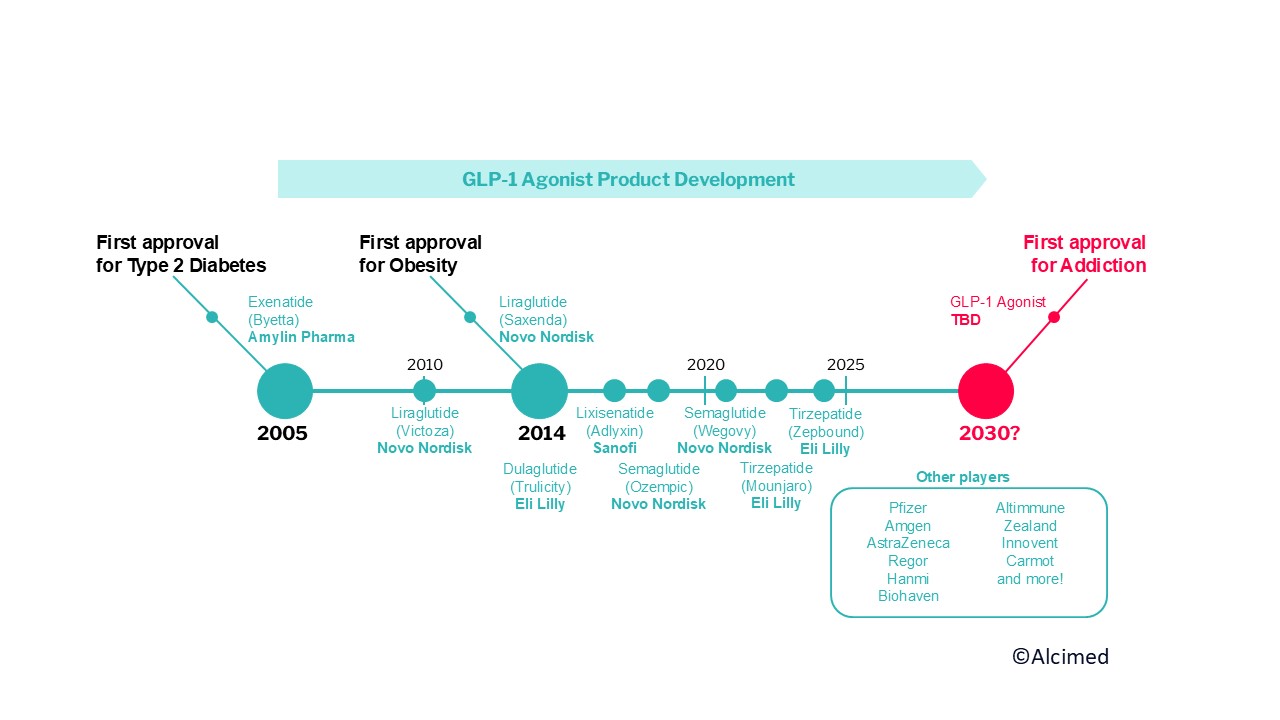
Following the 2005 approval of exenatide for Type 2 Diabetes, there have been a series of approvals for GLP-1 agonists in both diabetes and obesity. Semaglutide and tirzepatide dominate the current market and have made GLP-1 producers Novo Nordisk and Eli Lilly 2 of the top 3 pharma companies by market cap.
Ongoing efforts are aimed at developing next-generation GLP-1 agonists for obesity and other therapeutic areas. As of early 2025, well over 30 new GLP-1 drugs are in development. Current players are expanding their pipelines; for example, Lilly expects to share Phase 3 obesity data on orfoglipron, an oral GLP-1 agonist, and retatrutide, a triple agonist of GLP/GIP/glucagon receptors in 2025. More players ranging from large pharma (including Pfizer, Amgen and AstraZeneca) to growing biotechs are also hoping to carve a slice of the pie. Notable Series A funding efforts for new-to-the-scene biotechs with early phase assets include $410 million for Verdiva Bio in 2025 and $400 million for Kailera Therapeutics in late 2024.

Mechanisms of Action: From Obesity to Addiction
GLP-1 agonists enhance insulin secretion, slow gastric emptying, and promote satiety by acting on GLP-1 receptors in the hypothalamus and other brain regions involved in hunger regulation. This leads to reduced food intake and significant weight loss in clinical trials and real-world use.
Could they work for substance use disorders? GLP-1 agonists appear to influence reward-related pathways beyond appetite control. These drugs modulate dopaminergic signaling in the mesolimbic system, the brain’s reward circuit, which is also implicated in addiction. By dampening reward-driven behaviors, GLP-1 agonists could potentially reduce cravings and compulsive substance use.
- Real-world Evidence: There is mounting evidence that GLP-1 agonists administered for diabetes or obesity correspond to reduced addiction risk. A 2025 analysis found that GLP-1 agonists given for diabetes were associated with a reduced risk of substance use among hundreds of thousands of United States Veterans and a 2024 examination of over 500k patients found lower rates of opioid overdose and alcohol intoxication among patients that received a GLP-1 agonist. Similarly, a population-based study in Sweden found that individuals taking GLP-1 agonists for metabolic conditions had a lower incidence of alcohol-related disorders compared to matched controls. These large correlative epidemiological findings support a potential effect of GLP-1 on drug craving.
- Preclinical Research: Animal studies have demonstrated that GLP-1 agonists can reduce drug-seeking behavior in rodent models of cocaine and opioid addiction. These findings provide a mechanistic basis for the hypothesis that GLP-1 agonists could help curb addictive behaviors in humans.
- Early Clinical Results: In two small clinical studies, GLP-1 agonists reduced alcohol consumption and craving in patients with alcohol use disorder and reduced opioid craving by 40% among opioid use disorder patients.
While these results provide a robust basis for investigating GLP-1 agonist use in SUDs, there are some potential drawbacks that should be weighed. GLP-1 agonists can cause significant gastrointestinal side effects like nausea, vomiting, and diarrhea, along with risks of pancreatitis, gallbladder issues, and gastroparesis. They can also lead to muscle loss, which would be concerning for SUD patients if the off-target effects continue outside of obesity and diabetes.
Why Should We Care?
Despite advances in addiction medicine, FDA-approved pharmacotherapies for SUDs remain limited and have varying efficacy.
- Opioid Use Disorder (OUD): Medications like buprenorphine and methadone are effective but have barriers to access and adherence. GLP-1 agonists could be the first effective treatment for OUD that does not act on the opioid receptor pathway.
- Alcohol Use Disorder (AUD): Approved treatments such as naltrexone and acamprosate show modest efficacy, and many patients struggle with relapse.
- Stimulant Use Disorder: There are currently no FDA-approved pharmacotherapies for cocaine or methamphetamine addiction. Bupropion and varenicline are available for curbing nicotine use, but additions to the pharmacological toolkit can help the many individuals seeking more effective treatments.
With high relapse and overdose rates across substances, novel therapeutic strategies are urgently needed.
Find out how our team can support you in your market access strategies >
The Future of SUD Treatment
Beyond GLP-1 receptor agonists, several other pharmacological approaches are being explored for SUDs. Psychedelics, including psilocybin and MDMA, have shown promise for treating addiction by altering reward behaviors, but there is lasting uncertainty about the suitability of this drug class after the FDA denied approval for Lykos’ MDMA drug for PTSD in 2024. Additionally, monoclonal antibodies targeting substances like fentanyl are being developed to block their effects before they reach the brain, potentially reducing overdose risks. While these treatments remain in various stages of development, they highlight the growing recognition that novel, mechanism-driven therapies are needed to address addiction effectively.
GLP-1 agonists have already transformed the treatment landscape for diabetes and obesity, and their potential role in addiction medicine represents an exciting new frontier. If early-phase trials show promise, pivotal phase 3 studies could begin within the next few years, potentially leading to regulatory submissions later in the decade. We can help you explore this uncharted territory and strategize for success. Don’t hesitate to contact our team!
About the author,
Daniel, Healthcare Consultant in Alcimed’s Life Sciences team in the USA.